To bring this discussion even one step further, if you DO have an internal femur lengthening procedure, develop a valgum deformity, and notice in 2-3 (or 10) years your knees are feeling sore, particularly to the lateral compartment, you are not completely screwed. A femoral wedge osteotomy (removing a wedge of bone from the lower femur to reangle it) may straighten the knee. Doing so can at least partly reverse the damage being caused by the valgum to the lateral knee compartment. But it is not pleasant or easy.
Ref: http://emedicine.medscape.com/article/1251668-overview#aw2aab6b7
"The rationale of corrective osteotomy is to unload the diseased lateral compartment by overcorrecting the pathologic malalignment of the lower extremity and to facilitate the reparative capacity of the knee joint once it is mechanically unloaded. The regeneration of articular cartilage and proliferation of fibrocartilage has been demonstrated during repeat arthroscopy, compared with previous arthroscopic findings in knees that were overcorrected by an osteotomy.[39, 40, 41, 42, 43, 44, 45, 46]" (ie. Damage caused to the cartilage by genu valgum can repair itself to an extent once the genu valgum is corrected.)
"Valgus malalignment of the knee joint is often corrected by a distal femoral osteotomy, with a medial closing wedge fixed internally (see the image below)... It has been shown to be safe and effective in correcting deformity and slowing progression of knee arthritis. To bring the knee joint line parallel to the floor by osteotomy, the deformity usually has to be corrected in the deformed distal femur itself.[16, 42, 49, 52, 53, 54, 55, 56, 57, 58, 59, 60]" (ie. To properly fix this misalignment, you need to go back, chop off the lower end of the femur, take a small wedge out to reangle it, and then refix it together. Pic below. This will possibly cost you a small amount of height gain from all the sawing, plus it's another major operation you'd need on both sides, if someone is willing to even provide it to you for only a few degrees correction and after cosmetic LL sugery.)
The suggestion above of correcting it via tibial varusing during a tibial Ilizarov could also be valid. But then again, you need to do both upper and lower legs, and tibial Ilizarov isn't that much fun from what I gather. And again, you are opening yourself up to risk that your surgeon will not control the device precisely enough to give you the exact correction you need.
Seems better to me to just pursue methods of LL that don't (or at least more minimally) shift the axis of the hips/knees/ankles to begin with.
How LL (inevitably?) misaligns joints, creates x-legs, and causes joint pain
To bring this discussion even one step further, if you DO have an internal femur lengthening procedure, develop a valgum deformity, and notice in 2-3 (or 10) years your knees are feeling sore, particularly to the lateral compartment, you are not completely screwed. A femoral wedge osteotomy (removing a wedge of bone from the lower femur to reangle it) may straighten the knee. Doing so can at least partly reverse the damage being caused by the valgum to the lateral knee compartment. But it is not pleasant or easy.
Ref: http://emedicine.medscape.com/article/1251668-overview#aw2aab6b7
"The rationale of corrective osteotomy is to unload the diseased lateral compartment by overcorrecting the pathologic malalignment of the lower extremity and to facilitate the reparative capacity of the knee joint once it is mechanically unloaded. The regeneration of articular cartilage and proliferation of fibrocartilage has been demonstrated during repeat arthroscopy, compared with previous arthroscopic findings in knees that were overcorrected by an osteotomy.[39, 40, 41, 42, 43, 44, 45, 46]" (ie. Damage caused to the cartilage by genu valgum can repair itself to an extent once the genu valgum is corrected.)
"Valgus malalignment of the knee joint is often corrected by a distal femoral osteotomy, with a medial closing wedge fixed internally (see the image below)... It has been shown to be safe and effective in correcting deformity and slowing progression of knee arthritis. To bring the knee joint line parallel to the floor by osteotomy, the deformity usually has to be corrected in the deformed distal femur itself.[16, 42, 49, 52, 53, 54, 55, 56, 57, 58, 59, 60]" (ie. To properly fix this misalignment, you need to go back, chop off the lower end of the femur, take a small wedge out to reangle it, and then refix it together. Pic below. This will possibly cost you a small amount of height gain from all the sawing, plus it's another major operation you'd need on both sides, if someone is willing to even provide it to you for only a few degrees correction and after cosmetic LL sugery.)
The suggestion above of correcting it via tibial varusing during a tibial Ilizarov could also be valid. But then again, you need to do both upper and lower legs, and tibial Ilizarov isn't that much fun from what I gather. And again, you are opening yourself up to risk that your surgeon will not control the device precisely enough to give you the exact correction you need.
Seems better to me to just pursue methods of LL that don't (or at least more minimally) shift the axis of the hips/knees/ankles to begin with.
Quote from: maximize on April 10, 2015, 03:52:02 PMI think those of you with bowlegs (genu varum) are lucky. You might be the only "ideal" candidates for internal femurs in terms of potentially improving rather than worsening the mechanical axis.
Yeah I was fairly significantly bowlegged before (not ridiculously so, but it was noticeable if you looked enough at it), and now my legs are perfectly straight. And, I don't have x-legs when I stand with my feet apart. So if anything, I'm hoping the realignment has helped me a bit.
Quote from: maximize on April 10, 2015, 03:52:02 PMI think those of you with bowlegs (genu varum) are lucky. You might be the only "ideal" candidates for internal femurs in terms of potentially improving rather than worsening the mechanical axis.
Yeah I was fairly significantly bowlegged before (not ridiculously so, but it was noticeable if you looked enough at it), and now my legs are perfectly straight. And, I don't have x-legs when I stand with my feet apart. So if anything, I'm hoping the realignment has helped me a bit.
For anyone with unoperated, natural, well aligned knees who doubts or wonders how a subtle valgum would affect their hips/knees/ankles/gait, I suggest a simple experiment. It's not perfect, but I think it's the best you can do without actually operating on yourself.
Pick up a pair of cheap dollar store foam sandals. Cut a small wedge of foam off from the sandals to run along the whole outside of your feet like this:
Put the wedging material in your shoes. Now walk around with that for the next week or two. Maybe the next month or year. Do that and then report back how natural your gait now feels, and how naturally or not your knees and ankles hinge.
I just tried it for a few minutes, and I could be mistaken but I think I might have been starting to develop the same kind of subtly "strange" looking gait we have seen from some lengtheners that have done internal femurs. eg. Like the video that was posted ITT a bit earlier. Not sure. Could be placebo. It certainly feels different though.
I'm not suggesting performing this experiment will accurately emulate what happens from the shift in axis caused by internal femur lengthening surgery. The only thing that can show you what that would feel like would be to actually get the surgery and see. But I think it should make it evident if you try it that even subtle valgus stresses/deviations can change the mechanics quite noticeably.
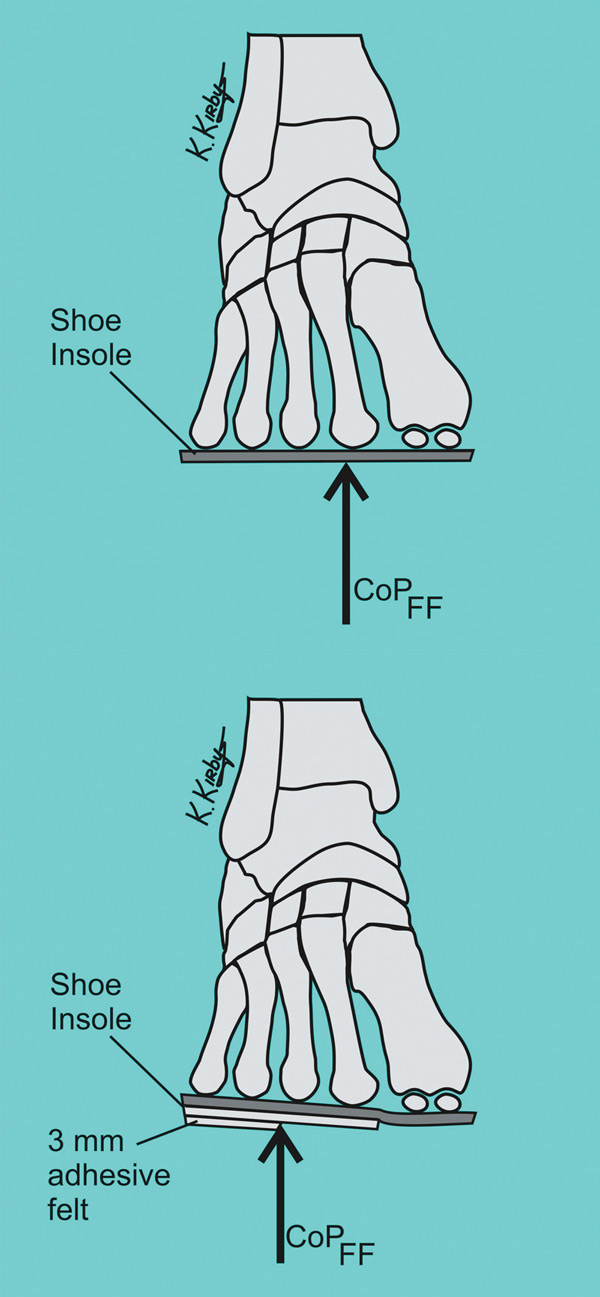
On the other hand, if you have already had internal femurs done and are experiencing knee/ankle pain, perhaps you may wish to try the opposite and apply a medial wedge (to the inside of your foot) to see if it helps relieve your discomfort like this: 
If it helps, custom orthotics can be designed with a medial wedge like this, and it may be the simplest, easiest method to manage any discomfort caused by the valgus shift.
Damn. You are making some good and important observations!
I was planning on lenghtening my femurs only 6cm because I was already concerned on biomechanical functionality due to the tibia to femur ratio and proportions.
I was sure I wanted to do femurs because i guess using aomething like 2cm insoles or boots would helph that ratio..
Unfortunately and from what you are saying using insoles or boota wouldn't make a different when it xomes to the problem you are pointing out... Or would it?
There god I will only do it in 4-5 years time when ll is way more expensive but more studies have been done.
What are your thoughts when it comes of using insoles to helph this voth cases after lenghtenig femurs? Would it help both, one of them or none?
Well at least when it comes to tibias using insoles or boots would only make things worse
this is getting tiresome and obessive
ask a surgeon.... a real dr what they think is best..
I just had another thought brainstorming solutions for this subject that I am finding exciting. In fact, it could be groundbreaking. Let me share. I hope you will find the concept as intriguing as I do. 
Current Internal Options:
Most of us would prefer to lengthen via internal fixation (eg. Guilet, Precision) for the speed, safety, and lack of wearing an external cage.
As stated, a internal tibial lengthening procedure should theoretically maintain the anatomical axis perfectly if well done. But when I was reviewing the journal articles on this, I was seeing even with this approach there can be slight deviations. It's understandable why, given that the exact angle of distraction will depend on the angle of the rod in the tibia. Drilling the rod into the tibia isn't exactly a perfect science, and a lot of tibias have a slight "S" curvature to them that could slightly alter the angle as the rod goes in. The point being, not even internal tibias will probably be "100%" perfect every time. But they should be pretty damn good. Tibia lengthening is slow though, and I'm not confident that a deformity couldn't occur to the fibula during distraction affecting the lateral ankle.
By contrast, internal femurs are fast, effective, and safe. Since only the femur is involved, there is minimal joint complexity. It's much easier to gain mechanical access to drill the hole for the device to be inserted (no patella, peroneal nerve, no fibula to fix, etc), so surgically it's as simple as can be. The problem is as stated, this approach guarantees that you will have axis deviation. Perhaps this may truly be a nonissue for many of us. But I think all of us would prefer not to have this axis deviation if there is a way to avoid it.
So what's my proposed solution? How can we improve the cutting edge of modern internal femur leg lengthening? Well I sort of brushed against the solution a bit earlier and I just connected it now. Some of you may perhaps think this is crazy, but bear with me. I think if you consider it fully, it may make a compelling argument.
Without further ado, here's my great big new idea ... Surgeons, if you like the idea, please feel free to apply liberally... Just please don't claim to name it after any one of you if it catches on... And please do PM me for co-authorship credits if you publish on it...
NEW IDEA - Internal Femur Lengthening Followed by Distal Femoral Opening Wedge Osteotomy (During Nail Extraction):
In my proposed new approach to lengthening, internal femur lengthening is first performed as usual. In this way, you get all the benefits of rapid growth, safety, and avoiding ankle/equinus/peroneal/patellar problems. You rehabilitate from this femur lengthening as usual for 1 year. When you reach the 1 year point and are ready to have your nail removed, final full leg sets of xrays are taken while standing in natural anatomical position. These xrays are then used to calculate and assess the degree of post-op genu valgum (or perhaps paradoxically varus if you have an abnormal alignment to begin with). The deviation is carefully assessed and measured for.
Then when you go in for your nail extraction, in addition to taking the nail out, if the misalignment is deemed significant, the surgeon performs a carefully calculated small bilateral distal femoral opening wedge osteotomy to perfectly correct it:

Re-alignment could be verified for perfection in the OR during the osteotomy with temporary pinning and portable xray before final fixation is applied. You can then get a rapid safe internal femoral lengthening, combined with a totally perfect (to the surgeon's skill level) correction of your axis bilaterally. Furthermore, since it's an opening wedge osteotomy, you don't lose a millimeter of height. In fact, you may actually gain a tiny bit more.
This adds one extra layer of surgery, but since it's done at the time of nail extraction, you're under anesthetic already anyway. The osteotomy procedure alos doesn't appear to be that complicated. Furthermore, it's rigidly fixed, so should be back to full normal weight bearing shortly post op. It could probably be optional whether or not you want the fixation metal for the osteotomy removed at a second follow up.
This could even provide superior alignment of the axis compared to internal tibias, because if you get a mild deviation during internal tibias, there is no way to correct that at the end. This approach offers a way to get a rapid femur growth and then completely fix any degree of misalignment no matter how great, as long as the finishing osteotomy is well planned and performed. In other words, if you can accept the idea of the osteotomy during nail removal, I think it's pretty much a perfect solution for rapid, safe femur lengthening while maintaining neutral knee/ankle axis alignment.
I'm pretty happy. I think this is an awesome solution that should be offered electively to any person who wants it done. I think this would be a great approach if a reputable surgeon could be convinced to consider it. I hope if they like it, they won't mind that it wasn't their idea first. 
Also, I wasn't going to say this, but if it helps add weight to further consideration of this idea (which I think could potentially be quite good), then I will say it. I am a real doctor. Not a surgeon, but yes a real doctor. During med school and residency, I assisted in the OR for numerous hip replacements, knee replacements, arthroscopies, etc., did tonnes of ortho exams, joint injections, casting fractures, etc., and assisted consults in numerous orthopedic surgery offices. So I have at least some limited background in orthopedics.
I'd still do external tibias all over again before doing them internally. At least if you go to a doctor that offers a Taylor Spatial Frame or a six-axis correction system like a hexapod, your doctor can do a perfect realignment with the computer software once the lengthening is complete.
To be honest when I was making my previous post I thought about it. But not like you did. Mine were:
1. doing the Distal Lateral Femoral Opening Wedge Osteotomy at the time of the LL operation. It was stupid because we didnt know how much we were going to lenght.
2. Doing long time after. As you said before 2-3 (or even 10) years later
The way you said it was just perfect. Doing it when removing the nail! But what would be the new risks? The new price?
You must be logged in to post a reply.